
This article is intended for anybody who is interested in learning about the role of a QME in California workers’ compensation.

Why is an attorney asking me for a deposition?
This article is for medical providers who have been called in to give a deposition on a workers’ compensation case.
Continue reading Why is an attorney asking me for a deposition?
3 tips to help you get paid for your PR-4 report
This article is intended for medical providers and other medical professionals.
When you complete a Permanent & Stationary PR-4 report, it can be difficult to get paid for the full and correct amount.
This article includes a few tips to help ensure that you get compensated for your report.
Continue reading 3 tips to help you get paid for your PR-4 report
What Are the Different User Levels in RateFast?
Each RateFast user has a User Level. Your User Level determines how much information you can access in your patients’ workers’ compensation report.
This article describes how to assign a user’s User Level, and what each User Level means.
Continue reading What Are the Different User Levels in RateFast?
How to Simplify ICD-10 Codes Using RateFast
As of October 1st 2015, U.S. medical providers are required to use ICD-10 codes instead of ICD-9 codes.
Although there are more than 70,000 new codes (many of which feature an overwhelming amount of specificity) we believe that this transition can—and should—be simplified with the help of medical software.
Continue reading How to Simplify ICD-10 Codes Using RateFast
What is Occupational Telemedicine?
Our sister website www.pr4report.com recently created a downloadable FAQ about telemedicine in workers’ compensation—or “Occupational Telemedicine.”
If you’re in workers’ compensation and you’d like to learn more about how you can use telemedicine—online visits—to benefit your practice and patients, then just this might be worth reading.
A lot of RateFast members use telemedicine in conjunction with RateFast to great effect. Contact us for more information about how telemedicine can benefit your medical practice.
Automatic billing for your PR-4 reports! How to use the RateFast Billing Calculator
Accurately sending your bill for a PR-4 report can be a time consuming process, but it doesn’t need to be.
The RateFast PR-4 Billing Calculator counts the amount of pages in your PR-4 report, asks some basic questions, and then prints out a bill at the end of your report.
This article describes how to turn on the billing calculator and how to use it correctly.
Continue reading Automatic billing for your PR-4 reports! How to use the RateFast Billing Calculator
ICD-10 Codes in RateFast
If you’re a medical provider in the U.S., then you know that on October 1st 2015 we will be switching from ICD-9 to ICD-10 codes. There are more than 100,000 new codes.
A lot of medical workers are concerned that the transition might be rocky, but RateFast users need not fear.
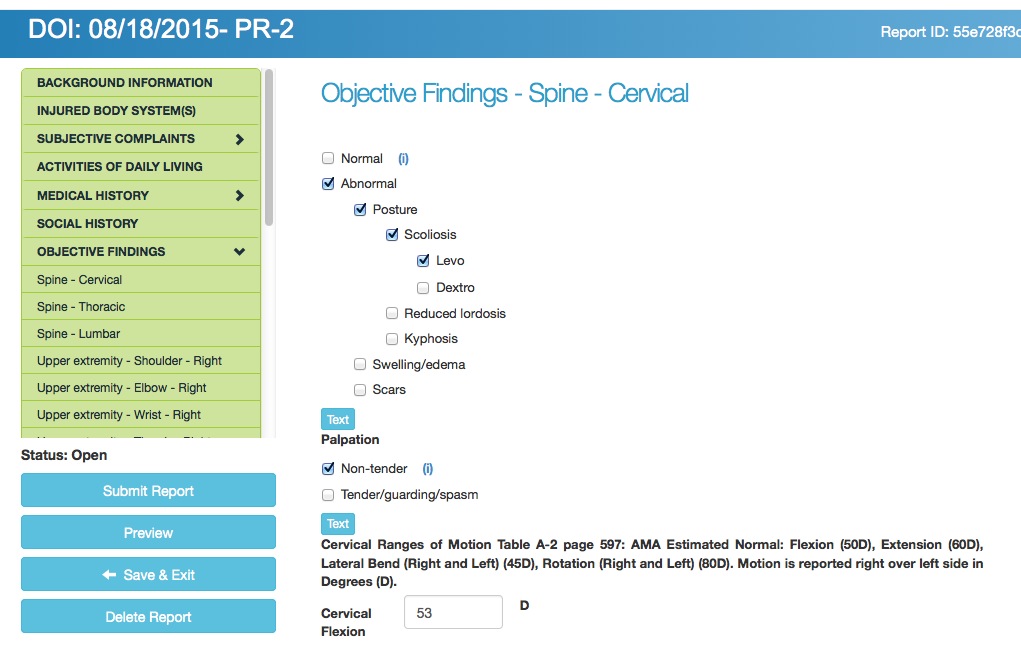
Completing the “Objective Findings” section in RateFast Reports
If you’re a current RateFast user, then you’ll recognize these exams from the “Objective Findings” section of your Doctor’s First, PR-2, and PR-4 reports.
All the information in the Objective Findings examinations should be, well, objective: any other medical provider should be able to examine the patient’s injury and come back with the same results.
Some parts of an Objective Findings examination require you to take measurements using various pieces of equipment (such as goniometers and inclinometers) or to perform different types of tests (such as distal neurovascular exams and monofilament testing).
Related Reading
Click here for a full list of the body part exams that are currently written into the RateFast application.

When should an injured worker get an attorney?
If you’re a medical provider in workers’ compensation, then sometimes your patients might want legal representation.
When your patients ask, “Should I get an attorney?” then we recommend referring them the Disability Evaluation Unit.
To learn why, listen to our podcast on the subject here: “Attorneys in Workers’ Comp: A Historical Perspective” (released September 3rd, 2015).
The DEU has offices in the following locations:
| Anaheim 1065 N. PacifiCenter Drive Anaheim, CA 92806 (714) 414-1803 |
Oxnard 1901 N. Rice Avenue, Suite 200 Oxnard, CA 93030 (805) 485-4423 |
San Francisco 455 Golden Gate Avenue, 2nd floor P.O. Box 420603 San Francisco, CA 94142 (415) 703-5030 |
| Bakersfield 1800 30th Street, Suite 100 Bakersfield, CA 93301-1929 (661) 395-2723 |
Pomona 732 Corporate Center Drive Pomona, CA 91768 (909) 629-6288 |
San Jose 100 Paseo de San Antonio, Room 223 San Jose, CA 95113 (408) 277-2024 |
| Eureka * Satellite office Ratings to be sent to Redding |
Redding 250 Hemsted Drive, Second Floor, Ste. B Redding, CA 96002 (530) 225-3179 |
San Luis Obispo 4740 Allene Way, Suite 100 San Luis Obispo, CA 93401 (805) 596-4157 |
| Fresno 2550 Mariposa Mall, Room 2005 Fresno, CA 93721-2280 (559) 445-6427 |
Riverside 3737 Main Street, 3rd floor Riverside, CA 92501 (951) 782-4345 |
Santa Ana 605 W Santa Ana Blvd, Bldg 28, Room 451 Santa Ana, CA 92701 (714) 558-4113 ext. 6749 |
| Long Beach 300 Oceangate Street, Room 325 Long Beach, CA 90802-4460 (562) 590-5017 |
Sacramento 160 Promenade Circle, Suite 300 Sacramento, CA 95834 (916) 928-3150 |
Santa Barbara * Satellite office Ratings to be sent to Oxnard |
| Los Angeles 320 W. 4th Street, 9th floor Los Angeles, CA 90013 (213) 576-7426 |
Salinas 1880 North Main Street, Suites 100/200 Salinas, CA 93906-2204 (831) 443-3222 |
Santa Rosa 50 “D” Street, Suite 420 Santa Rosa, CA 95404 (707) 576-2374 |
| Marina del Rey 4720 Lincoln Blvd 2nd floor Marina del Rey, CA 90292 (310) 482-3868 |
San Bernardino 464 W. Fourth Street, Suite 260 San Bernardino, CA 92401 (909) 383-4522 |
Stockton 31 East Channel Street, Room 417 Stockton, CA 95202-2314 (209) 948-3651 |
| Oakland 1515 Clay Street, 6th floor Oakland, CA 94612 (510) 622-2859 |
San Diego 7575 Metropolitan Drive, Suite 202 San Diego, CA 92108 (619) 767-2081 |
Van Nuys 6150 Van Nuys Blvd., Room 200 Van Nuys, CA 91401-3373 (818) 901-5376 ext. 5 |